



Last week I argued that healthcare doesn’t need more AI tools — it needs an architecture, and I called that framework Operations-First AI. It’s the why: build from the operations up, not the algorithm down.
The response I got most was a fair one: “Okay. I’m convinced. How do I actually get there?”
That is the right question, and this is the answer. Becoming AI-native is not a switch you flip or a tool you buy. It is a climb, and it has stages. Here is the map.

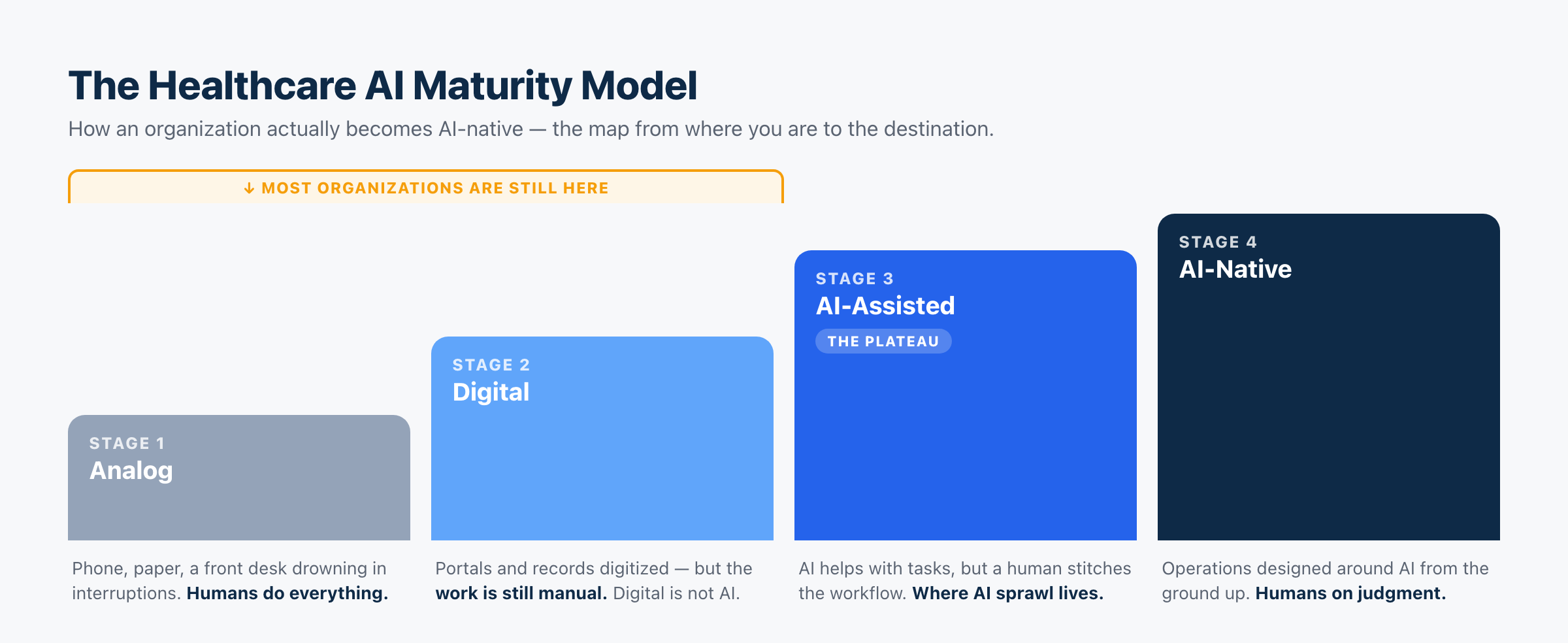
Four stages, and the honest truth is that most organizations — from a two-provider clinic to a national health system — are sitting on the first two, convinced they are further along than they are. Let me define each one, because the difference between them is the difference between spending money on AI and actually becoming AI-native.
Stage 1 — Analog
People are the workflow.
The phone rings and a human answers, or it doesn’t and rolls to voicemail. Intake is on paper or typed by hand. The front desk is interrupted all day, closed half of it, and English-only in a country that isn’t. Every task depends on a human being available and unbusy at the exact moment it’s needed.
This is more common than the industry likes to admit. Plenty of practices have a modern website and still run their actual operations analog. If your schedule lives in one system, your calls in a person’s memory, and your follow-up in a sticky note, you are here — no matter how new your logo is.
Stage 2 — Digital
The information is digital; the work is still manual.
Records are digitized. There’s an EHR, a patient portal, maybe online forms. This feels like modernization, and it is a real improvement over paper. But look closely at the work: it is still manual. A human still answers the phone, still enters the data, still chases the no-show, still stitches the day together by hand. The information got digital. The labor didn’t.
This is the most dangerous stage, because it is the easiest to mistake for the destination. Digital is not AI-native. Most organizations that think they’ve modernized have only digitized. They have better filing cabinets and the same overloaded front desk.
Stage 3 — AI-Assisted (the plateau)
AI helps; humans still orchestrate.
Now AI enters — as help. A scribe drafts the note. A bot answers a few FAQs. A tool sends recall texts. Each one genuinely lifts a little weight. This is where most self-described “AI adopters” actually are.
And it is where they get stuck. Because AI-assisted is exactly where AI sprawl lives: a pile of point tools, each automating its own task, none of them connected, a human still stitching the workflow together between them. The practice has more AI than ever and is not meaningfully more capable, because the tools don’t compound. Adding a tenth assistant doesn’t get you to the next stage. It just deepens the pile.
This is why I call Stage 3 the plateau: it feels like arrival and it is actually a trap. The jump from Stage 3 to Stage 4 is the hard one, and it is not a jump in capability. It is a jump in architecture.
Stage 4 — AI-Native
AI orchestrates; humans provide judgment.
Stage 4 isn’t what happens when you buy one more AI product. It’s what happens when AI stops being another tool and becomes part of how the organization operates.
An AI-native organization did not bolt AI onto its operations. It designed its operations around AI. The front office, scheduling, intake, follow-up, and communication run as one connected system that acts on its own and escalates to a human when judgment is required. People are deliberately placed where they add the most — judgment, empathy, ambiguity, and every clinical decision — instead of on data entry and phone tag.
This is the destination, and almost no one is there yet. That’s not a failing; it’s the opportunity. AI-native isn’t about having the most AI. It’s about having an architecture — which is why an organization can be drowning in AI tools (Stage 3) and still not be AI-native.
The rungs are architectural, not technological
Here is the pattern that matters. Every jump up this ladder looks like it should be about technology, and none of them actually are.
Analog to Digital feels like buying software; really it’s a shift in where information lives. Digital to AI-Assisted feels like buying AI; really it’s the start of offloading tasks. And the biggest jump — AI-Assisted to AI-Native — isn’t about buying anything at all. It’s about connecting what you have into a system with a design: what talks to what, who decides what, where the human steps in. Where you sit on this ladder is a question of architecture, not capability.
And notice what that really makes this: a model of organizational maturity, not technological maturity. The rungs don’t measure how much AI you own — they measure how much of your organization has been redesigned around it.
Organizations don’t become AI-native by buying more AI. They become AI-native by redesigning how work happens.
The models are a commodity; the redesign is the hard, durable work — which is exactly why it’s defensible.
This reframes the whole “are we behind on AI?” anxiety. Most organizations are not behind because they lack access to good models — the models are a commodity now. They are stuck at Stage 2 or 3 because they never built the architecture that turns tools into a system. That’s also why the research keeps finding that most AI projects stall before they scale: the blocker isn’t the AI, it’s everything around it. Bain’s work with KLAS frames the whole industry as finally moving “from pilot to production,” and the ones that make it are the ones that stopped collecting tools and started building operations (Bain). Deloitte describes the same split as an “AI divide” between organizations embedding AI into their operating model and those leaving it as scattered point solutions (Deloitte) — which is, precisely, the gap between Stage 3 and Stage 4.
Where are you, really?
A quick, honest self-assessment. Ask:
- When a patient calls after hours, what happens? (Voicemail → Stage 1–2. A system that helps and captures → 3–4.)
- If your best front-desk person is out sick, does the operation degrade? (Yes → you’re running on people, not architecture.)
- Count your AI tools. Now ask how many talk to each other. (Many tools, no connections → Stage 3, sprawl.)
- When AI handles something, does a human still have to re-key it somewhere? (Yes → assisted, not native.)
- Could a patient move from call to booking to reminder to recall without a staff member manually carrying them between steps? (No → you haven’t crossed into Stage 4.)
- If you removed every AI tool tomorrow, would the operation run about the same? (Yes → the AI is decorative, not architectural — a Stage 3 tell.)
Most readers will land on Stage 2 or early Stage 3. That is not a problem to be embarrassed about. It is a map with a clearly marked “you are here.”
The same ladder, at every scale
This model is not just for small practices. A national health system and a public payer climb the identical four rungs — most of them are also stuck at Digital or AI-Assisted, drowning in point solutions and pilots, with the same unbuilt architecture underneath. The scale changes the size of the climb, not its shape. The implementation changes. The principles don’t.
And the route up is always the same: Operations-First. You do not become AI-native by starting with the most sophisticated clinical model. You become AI-native by building the operational foundation first, then designing everything else to run on it. The place to start that climb is the front office — the highest-volume, most measurable, most deployable rung of the operational layer, and the one patients actually touch. I make that specific case in The AI Front Office — the layer we build at Viva AI, and the first real step from Stage 3 to Stage 4.
The bottom line
Operations-First AI tells you why and in what direction to build. The Maturity Model tells you where you are and how far you have to climb.
Put them together and the path is clear. Most organizations are lower on this ladder than they think, stuck not because they lack AI but because they never built the architecture to connect it. The climb from a pile of tools to an AI-native operation is the defining work of the next decade of healthcare — and it starts by being honest about which rung you’re standing on.
Every healthcare organization can move up this ladder. The question was never whether you’ll adopt AI — everyone will. It’s whether you’ll stop at AI-Assisted, where most do, or keep climbing all the way to AI-Native.
Frequently asked questions
What is the Healthcare AI Maturity Model?
It’s a four-stage map of how a healthcare organization evolves toward being AI-native: Analog (everything manual), Digital (records digitized but work still manual), AI-Assisted (AI helps with individual tasks but a human stitches the workflow), and AI-Native (operations designed around AI, humans placed on judgment). It’s the companion to Operations-First AI: the framework says why and in what direction to build; the maturity model says where you are and how far you have to climb.
What’s the difference between “digital” and “AI-native”?
Digital means your information has been computerized — an EHR, a portal, online forms. AI-native means your operations were designed around AI, so the work itself is automated and connected, not just the records. Most organizations that believe they’ve modernized have only digitized; the labor is still manual. Digital is Stage 2; AI-native is Stage 4.
Why is “AI-Assisted” a trap?
Because it feels like progress while quietly stalling you. At Stage 3 you accumulate disconnected AI tools (“AI sprawl”) that each automate a task but don’t connect, so a human still stitches the workflow together and the tools never compound. Adding more tools deepens the pile instead of advancing you. The jump to AI-Native is architectural — connecting what you have into a system — not buying another assistant.
How do I know which stage my organization is on?
Ask what happens to an after-hours call, whether the operation degrades when a key staffer is out, how many of your AI tools actually talk to each other, and whether a patient can move from call to booking to reminder without a human carrying them between steps. If humans are manually bridging the gaps, you’re at Stage 2 or 3, regardless of how much software you own.
Does the maturity model apply to large health systems and payers?
Yes. Health systems and payers climb the same four rungs, and most are also stuck at Digital or AI-Assisted — drowning in pilots and point solutions with the architecture still unbuilt. The scale of the climb changes; the stages don’t.
How does an organization move up the ladder?
By building Operations-First: modernize the operational foundation before layering on more sophisticated AI, and design the pieces to connect into one system rather than accumulating tools. In practice the first step from Stage 3 to Stage 4 is usually the front office — the highest-volume, most deployable part of operations.
Read next
- Why Healthcare Needs an AI Architecture (Not More AI Tools)
- The AI Front Office
- AI in Healthcare: A Builder’s Guide to What Actually Works
- AI in Healthcare: Real Examples That Work Today
- AI Voice Agent Architecture: What I Learned Building the Same Agent Three Times