By every conventional measure, the large health system should be healthcare’s AI leader. It has the budget, the data science team, the innovation office, the academic partnerships, the sheer volume of data. If AI maturity tracked resources, the health system would be at the top of the Maturity Model and the solo practice at the bottom.
It usually doesn’t. My prediction is the reverse: the large health system will sit at the AI-Assisted plateau longer than almost any other kind of organization, and many will be quietly overtaken by practices a fraction of their size. The organization with the most AI in healthcare is often the least AI-native — and the reason is specific, structural, and mostly invisible to the people inside it.
Why the biggest is the most stuck
The health system’s problem is not that it lacks capability, talent, or will. It’s that the organization is superbly engineered for one kind of change — and AI-native transformation is the other kind.
A health system is built to change carefully. Its entire apparatus — committees, evidence review, risk controls, staged rollout, sign-off at every level — exists because it makes decisions where being wrong can kill someone. That machinery is not bureaucracy for its own sake. For clinical decisions, deliberate and governed change is exactly right.
But operational change has the opposite requirements. Modernizing the front office, connecting the operating layer, redesigning how patients get scheduled and followed up — that work rewards speed, ownership, and iteration. And when you run it through the clinical-grade machinery, the machinery doesn’t protect it. It paralyzes it.
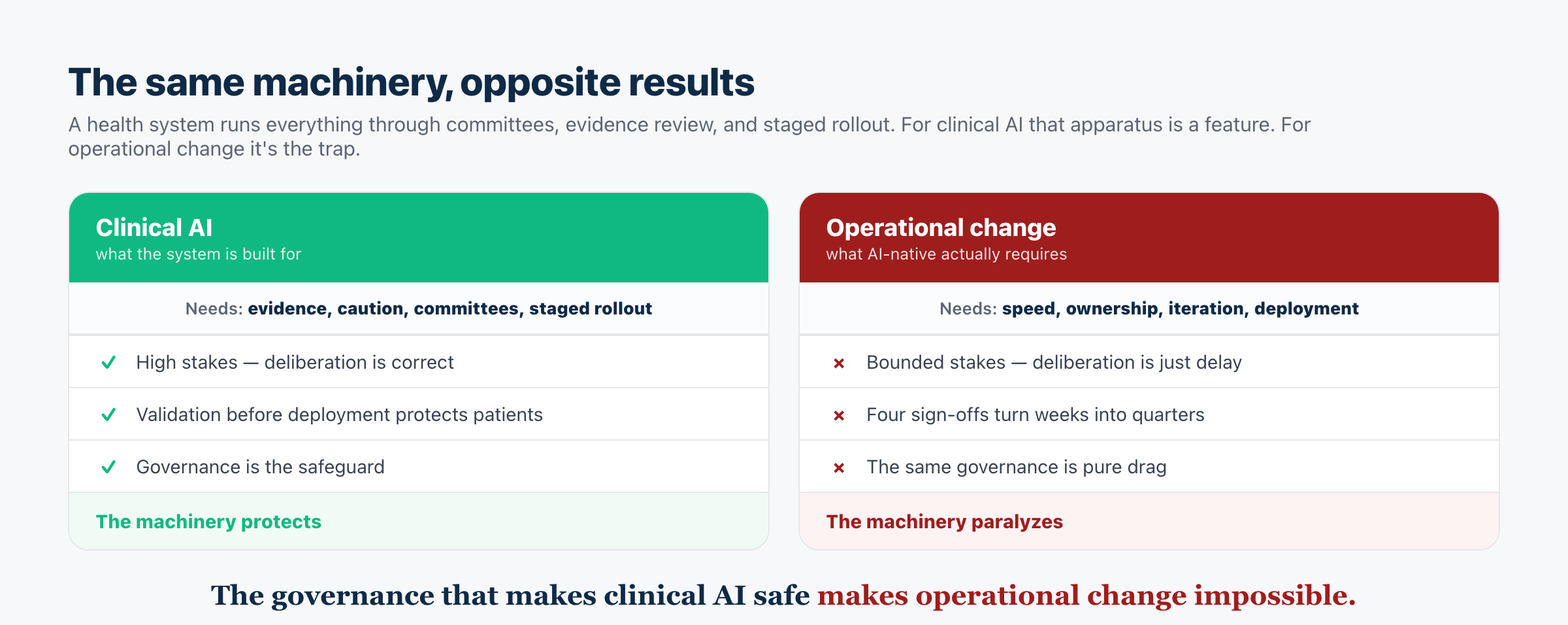
This is the trap in one line: the governance that makes clinical AI safe makes operational change impossible. A two-person practice can decide to rebuild its front office on Tuesday and be live the following week. A health system routes the same decision through IT, clinical leadership, compliance, security, and finance, each on its own calendar, and what should take days takes quarters — for a change that carries none of the clinical risk the process was designed to guard against.
Layer on the rest of the plateau, in its most entrenched form. The integration backlog is measured in years and dozens of systems. The operating layer is split across so many departments that no one owns it end to end. And the system’s clinical mission pulls its AI ambition toward the exam room first — building diagnostic AI on top of an operational base that can’t reliably get the patient there, which is building the roof before the foundation at the largest possible scale. The health system doesn’t plateau for lack of AI. It plateaus because everything that makes it good at medicine makes it slow at operations.
What actually gets a health system off the plateau
The prescription follows from the diagnosis, and it’s uncomfortable because it runs against instinct.
Stop governing operational change like a clinical intervention. The single highest-leverage move is to recognize that redesigning the front office is not a clinical decision and should not go through the machinery built for clinical decisions. Carve operational transformation out of the committee apparatus and give it a different, faster process — one built for reversible, bounded, non-clinical work. The governance is correct for the exam room and wrong for the phone line; stop applying the same reflexes to both.
Name a single accountable owner of the operating layer. This is the one prescription where the health system’s scale is an advantage rather than a liability: unlike a small practice, it can genuinely justify a dedicated owner of the operating layer with real authority across departments. Used well, that role is how a system converts its resources back into an advantage.
Sequence operations before clinical AI. The clinical moonshots will pay off far more once they sit on an operational layer that actually works. Modernize the foundation first, even though the prestige and the mission both pull the other way.
Change the scoreboard. As long as success is measured in pilots launched and papers published, the system will keep generating AI Sprawl and calling it progress. Measure operational outcomes instead — access, time-to-appointment, recovered contacts, staff time returned.
The prediction
Here is the falsifiable version. The health systems that break out of Stage 3 first will not be the ones with the biggest AI budgets, the most data scientists, or the most-cited research. They’ll be the ones that did something unglamorous: put one accountable owner on the operating layer, pulled operational change out of the clinical-governance apparatus, and shipped a single connected patient-access system before their next diagnostic-AI pilot.
The tell to watch for is a shift in what a system talks about. Today the leaders announce pilots and partnerships. The ones actually climbing will start reporting operational outcomes — missed calls recovered, time-to-third-available-appointment, no-show rates, access for non-English-speaking patients. When a health system stops counting models and starts counting whether patients can get in, it has left the plateau.
The bottom line
The health system’s predicament is almost tragic: the very qualities that make it excellent — caution, rigor, governance, a bias toward evidence over speed — are the ones holding it at the plateau. None of those qualities are wrong. They’re simply aimed at the wrong layer.
Becoming AI-native doesn’t require a health system to abandon what makes it safe. It requires drawing a line between the layer where careful, governed change is a virtue and the layer where it’s a liability — and letting operations move at operational speed. Until it draws that line, the biggest organization in the market, with the most AI money can buy, may keep losing the AI-native race to the independent practice down the road that simply decided to move.

Frequently asked questions
Why would a large health system be less AI-native than a small practice?
Because AI maturity is bottlenecked by organizational change, not resources — and a health system is engineered for careful, governed, evidence-based change, which is correct for clinical decisions and fatal for operational ones. Its committees, integration backlog, and split ownership turn an operational change that should take weeks into one that takes quarters. A small practice, with none of that drag, can simply move.
Isn’t rigorous governance a good thing in healthcare?
Yes — for clinical decisions, where being wrong can harm patients, deliberation and validation are essential. The mistake is applying that same clinical-grade machinery to operational change, which is bounded, reversible, and non-clinical. The governance that protects the exam room paralyzes the phone line.
What’s the single most important thing a health system should do?
Recognize that operational transformation is not a clinical intervention and stop governing it like one — carve it out of the committee apparatus and give it a faster, ownership-driven process. Then name a single accountable owner of the operating layer (something a system, unlike a small practice, can genuinely resource) and sequence operations before clinical AI.
How can you tell if a health system is actually making progress?
Watch what it reports. Announcing pilots, partnerships, and published models is plateau behavior. Reporting operational outcomes — recovered missed calls, time-to-appointment, no-show reduction, access for underserved patients — is the sign a system has stopped counting AI and started deploying it.
Does this mean health systems can’t reach AI-Native?
They can, and their resources become a real advantage once the binding constraint is removed. But the constraint isn’t money or talent — it’s the organizational machinery. A health system reaches AI-Native by separating operational change from clinical governance and giving the operating layer an owner, not by spending more on AI.
Read next
- Why Independent Practices May Reach AI-Native First
- Why DSOs Mistake Scale for Maturity
- Why Organizations Plateau at AI-Assisted
- Who Owns the Operating Layer?
- The Healthcare AI Maturity Model