The phone is still the front door to most medical and dental practices.
That sounds old-fashioned, but it is still true. Patients call to schedule, reschedule, ask about insurance, explain a concern, follow up after treatment, pay a balance, cancel, confirm, or figure out whether they should come in at all. Some text. Some use web chat. Some email. But the front office is still the layer where a patient turns intention into care.
And that layer is more fragile than most people realize.
The front desk is interrupted all day. Calls come in while staff are checking in patients, explaining forms, collecting payments, helping the clinical team, and managing whatever just walked through the door. Patients call after hours. They wait on hold. They land in voicemail. They speak different languages. They forget details. They are anxious. They ask one thing and then switch to another. They need help, but the system around the practice is often too overloaded to respond well.
This is where conversational AI in healthcare becomes real.
Not because AI can sound human.
That part is no longer the most interesting problem.
The real question is whether AI can operate the front door of a healthcare practice with enough reliability, safety, and integration that a real team can trust it with patients.
I have built conversational AI for dental front offices. That gives me a very specific bias: I care much less about demos and much more about what happens when a worried patient calls on a bad connection, switches languages mid-sentence, gives an unusual name, asks about a bill, tries to reschedule, and expects the practice to actually do something.
This post is about what I think is becoming one of the first real categories of conversational AI in healthcare:
The AI front office.
Not a chatbot.
Not voicemail with a better voice.
Not an answering service.
A real operational layer between patients and care.
I have written the broader version of this argument in AI in Healthcare: A Builder’s Guide to What Actually Works, and I have listed other real examples of AI in healthcare that work today. This article goes deeper on the front office because I think it is one of the clearest places where the research, the product opportunity, and the real-world deployment evidence all point in the same direction.
Patient access is not abstract. It starts with whether someone can get through.
Healthy People 2030 cites the National Academies definition of access to health care as the “timely use of personal health services to achieve the best possible health outcomes.” That definition matters because it makes access more than a policy word. Access is not just insurance coverage. It is not just the existence of a provider. It is whether a patient can actually use care when it matters.
Source: Healthy People 2030 — Access to Health Services
That is why the front office matters.
A patient who cannot reach the office does not have access in any practical sense. A patient who gives up after a long hold does not have access. A patient who cannot communicate in their language does not have access. A patient who gets a reminder too late, or no follow-up at all, may miss the care they intended to receive.
The research matches what I see in practices.
A Kyruus Health consumer access report found that despite growing interest in digital self-service, consumers still cited phone scheduling as their top preference for booking medical appointments. But the phone channel often failed them: less than half were able to schedule on the first call into a healthcare call center, about one in five reported long hold times, and among those who experienced long holds, close to 30% either could not book on the second try, went to another organization, or delayed care.
Source: Kyruus Health — Patient Access Journey Report
That is not a minor operational inconvenience. That is a failure at the access layer.
This is why I think the “front office” is the wrong name for the job. It sounds administrative. In reality, it is the access infrastructure of the practice.
Why the front office is the right first layer for healthcare AI
Most AI healthcare headlines focus on diagnosis.
That is understandable. Diagnosis is more exciting. AI reading scans, finding disease, recommending treatment, and assisting clinicians is important work. But it is also high-stakes, slow to validate, deeply regulated, and hard to deploy into daily clinical workflow.
The front office is different.
It is repetitive, high-volume, measurable, and mostly non-clinical. It is full of work that must happen correctly but does not require an AI system to make medical decisions.
The front office answers calls, schedules appointments, sends reminders, handles cancellations, collects payments, captures intake, routes urgent issues, reactivates patients, follows up after missed visits, and helps people in the language and channel they are comfortable using.
These tasks are not glamorous.
But they are where care begins.
They are also exactly the kind of tasks where automation has already shown value. A Cochrane review of mobile phone messaging reminders found that text reminders improved attendance at healthcare appointments compared with no reminders, and had a similar effect to phone call reminders while costing less in the studies that reported cost.
Source: Cochrane — Mobile phone messaging reminders for attendance at healthcare appointments
That is the broader lesson: small operational communication improvements can change whether patients show up.
A reminder is not clinical AI. Scheduling is not clinical AI. Follow-up is not clinical AI. But they change access, attendance, workload, and revenue. They also happen at a scale that humans struggle to sustain manually.
This is why I believe healthcare AI is paying off first in operations.
Not because clinical AI is unimportant.
Because operational AI is deployable now.
The AI front office is not a voice agent
One mistake people make is thinking this category is about voice.
Voice matters, but voice is only one channel.
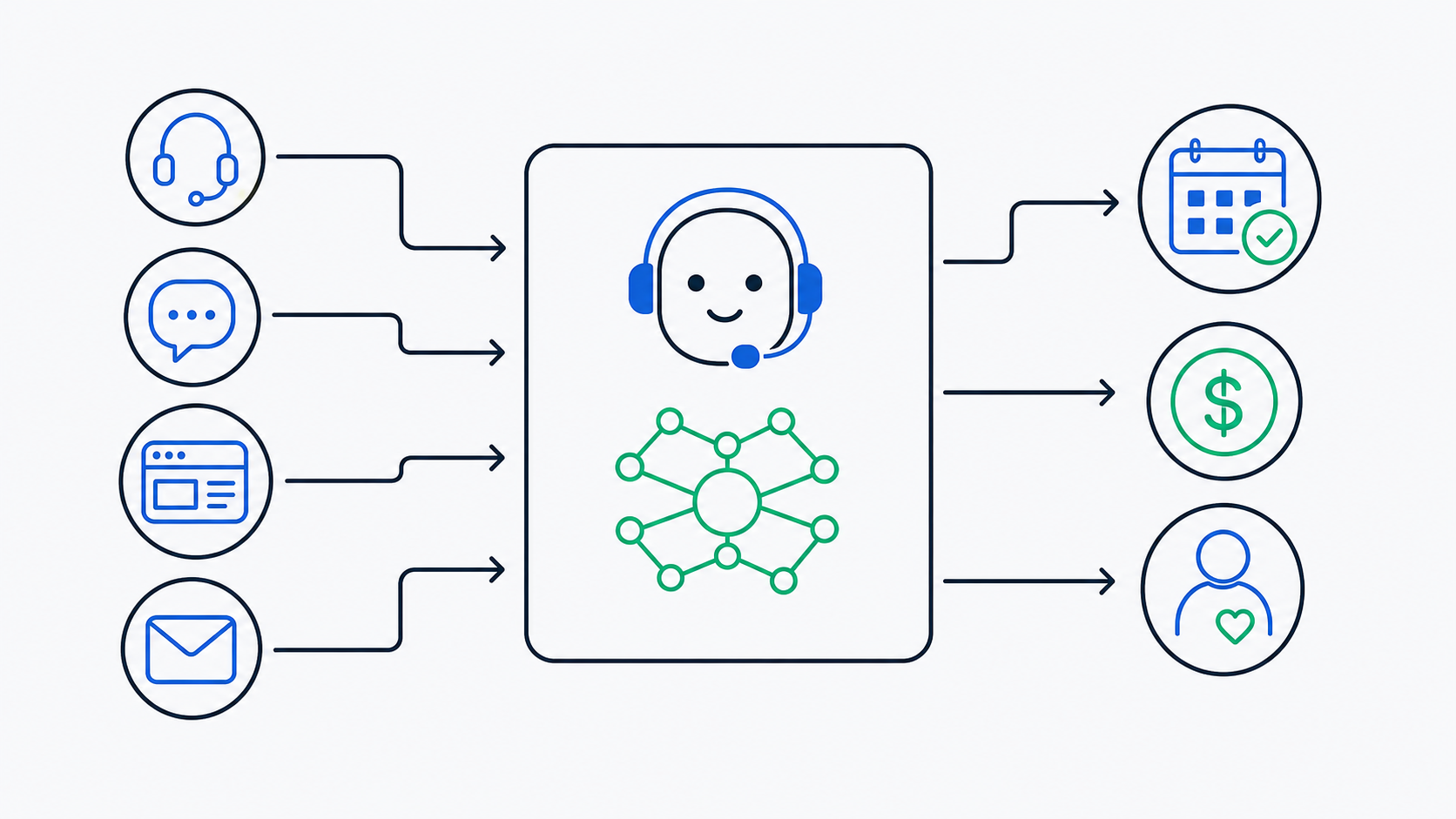
A real AI front office needs to handle phone, text, web chat, email, reminders, recalls, payments, and handoffs as one connected system. Patients do not experience a practice as a set of disconnected channels. They experience it as one relationship.
A patient might call on Monday, text on Tuesday, and reply to an email on Wednesday. The assistant should know the context. The office should not have four disconnected bots pretending to be one system.
The product is not the voice.
The product is the operational brain behind the conversation.
That distinction matters because a voice-only assistant can sound impressive and still fail at the job. If it cannot book into the real schedule, it is not a front office. If it cannot update the system, it is not a front office. If it cannot preserve context across channels, it is not a front office. If it only takes messages for staff to handle later, it has not removed the bottleneck; it has simply repackaged it.
A healthcare front office does not just talk.
It does work.
A real AI front office has five layers
After building this in practice, I think the AI front office has five layers.
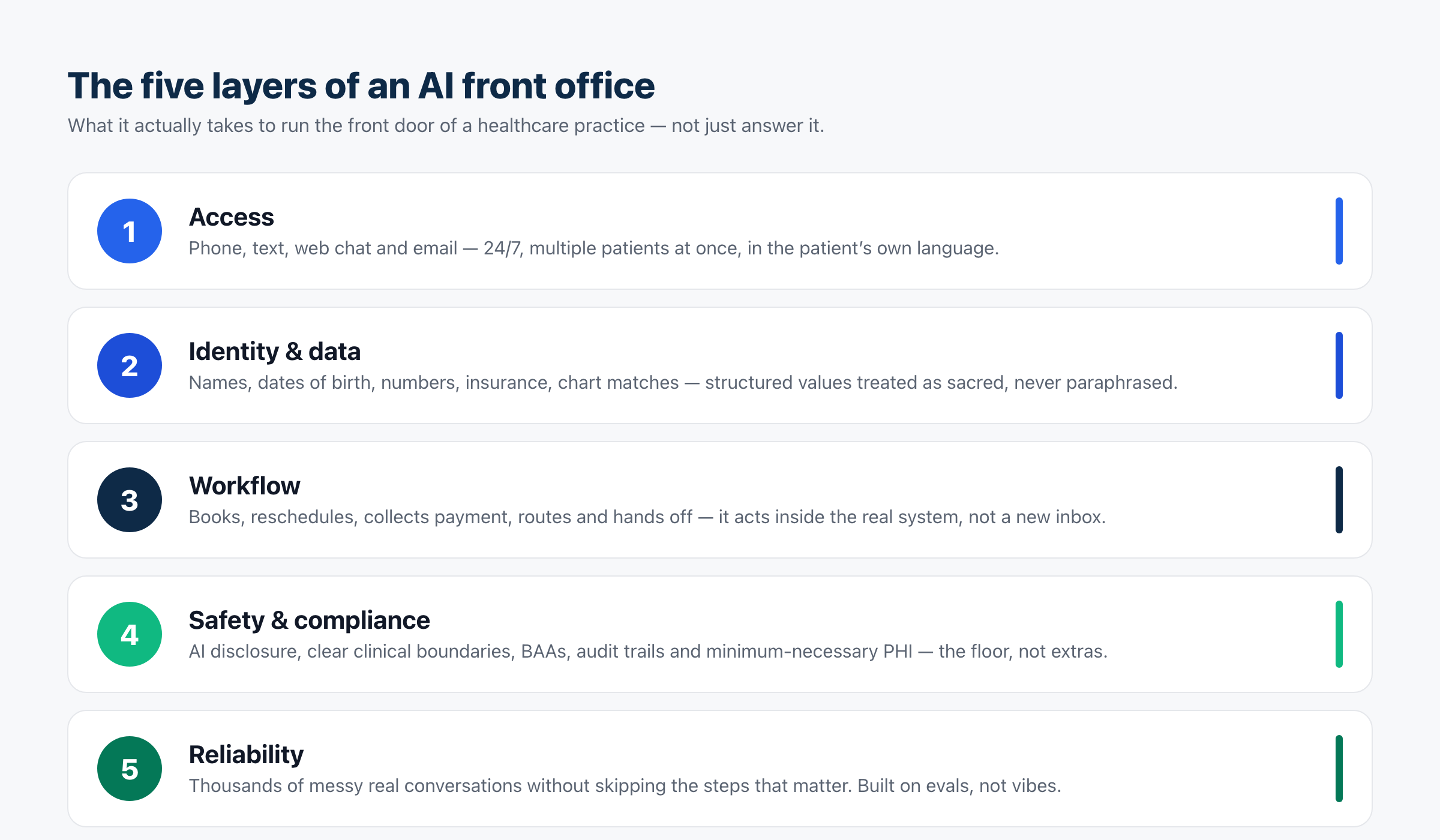
1. The access layer
This is the part patients see first.
The assistant answers calls, texts, web chats, and emails. It works after hours. It handles multiple patients at once. It supports patients in the language they are most comfortable using.
Language access is not a corner case. KFF estimated that in 2021, 25.7 million people in the United States, or 8% of people ages five or older, had limited English proficiency. HHS has also emphasized that language access is both a legal obligation and necessary for patient care, noting that roughly 68 million people in the U.S. speak a language other than English at home and that language barriers can affect quality and outcomes.
Sources: KFF — Health Coverage and Care for Individuals with Limited English Proficiency and HHS OCR — Section 1557 Language Access Provisions
In a practice, this means multilingual AI is not a “nice feature.” It is part of access.
But the bar is higher than translation. The system has to detect the language, stay in that language, switch when the patient switches, and preserve the same safety and accuracy guarantees across languages.
An English-first system with translation bolted on is not enough.
2. The identity and data layer
A front office lives or dies by details.
Names. Dates of birth. Phone numbers. Appointment times. Providers. Insurance information. Balances. Treatment history. Chart matches. Consent. Referral sources.
These are exactly the details AI systems often handle too casually.
A model may round a time. Speech recognition may misunderstand a name. A transcript may look clean but confuse “fifteen” and “fifty.” A patient may spell a name once and pronounce it differently later. The assistant may summarize the conversation beautifully but miss the one field the office actually needed.
In a consumer chatbot, that is annoying.
In healthcare operations, it breaks the workflow.
A real AI front office treats structured values as sacred. It does not paraphrase 2:20 into “around two.” It does not confidently match the wrong patient. It does not end a call without the required information. It knows when to confirm naturally and when to slow down because accuracy matters more than speed.
This is where demos hide the hard part.
A demo shows a natural conversation.
A real system has to turn that conversation into clean, structured, usable data.
3. The workflow layer
This is where most conversational AI products fail.
They can talk, but they cannot do the work.
A real front office has to act inside the practice workflow. That means it can check availability, book appointments, reschedule, send confirmations, collect payments, route messages, log conversations, and create a clean handoff for staff.
If the assistant only captures a message for a person to handle later, it has not solved the problem. It has created a new inbox.
The workflow layer is also where the economics become clear. CAQH’s 2025 Index, summarized by AJMC, found that more than $20 billion in cost savings could be achieved through more adoption of automated and electronic workflows in U.S. healthcare. The report covered data from 600 provider organizations and health plans representing 63% of insured lives, and specifically pointed to manual workarounds as a source of burden, error risk, and slower reimbursement.
Source: AJMC — CAQH Index Finds $20 Billion in Cost Savings Opportunities
The AI front office sits directly in this theme. It is not only about patient convenience. It is about replacing manual, repetitive operational work with integrated workflows that move at the speed patients expect.
4. The safety and compliance layer
The safest healthcare AI products are often the ones with the clearest boundaries.
For the AI front office, my boundary is simple:
AI handles operations and communication. Clinicians make clinical decisions.
The assistant can book the visit. It can collect the reason for the visit. It can route an urgent caller. It can help a patient understand office policies, appointment availability, payment options, or what information to bring.
It should not diagnose.
It should not independently triage symptoms.
It should not tell a patient whether something is serious.
It should not change treatment recommendations.
It should not improvise clinical advice.
It also has to be honest about what it is. It should disclose that it is AI. It should not pretend to be a nurse, doctor, or human receptionist. It should not make promises the office did not authorize.
Healthcare AI also touches protected health information very quickly. HHS explains that a business associate is an entity performing functions or services involving the use or disclosure of protected health information on behalf of a covered entity, and that covered entities must obtain written satisfactory assurances that the business associate will safeguard the PHI.
Source: HHS — Business Associates
That means Business Associate Agreements, audit trails, encryption, role-based access, minimum-necessary data handling, and deletion policies are not enterprise extras. They are the floor.
The same applies to AI trust. NIST’s AI Risk Management Framework describes trustworthy AI systems as valid and reliable, safe, secure and resilient, accountable and transparent, explainable and interpretable, privacy-enhanced, and fair with harmful bias managed.
Source: NIST — AI Risks and Trustworthiness
For healthcare conversational AI, those are not abstract values. They show up in the product details: what the assistant is allowed to say, what it is allowed to do, what it logs, what it escalates, how it handles language access, how it protects PHI, and how its failures are found before patients experience them.
5. The reliability layer
Reliability is the whole product.
Not the voice.
Not the prompt.
Not the demo.
Reliability.
A practice does not need an assistant that works once in a polished recording. It needs an assistant that can handle thousands of messy conversations without quietly skipping the steps that matter.
Real patients do not follow scripts. They interrupt. They change languages mid-sentence. They ask about insurance and then switch to pain. They give a wrong phone number and then correct it. They call from a noisy car. They ask about their child’s appointment and their own appointment in the same conversation.
This is where traditional software instincts break down.
You cannot script your way to reliability, because scripts break the moment a real patient leaves the expected path. But you also cannot let the model improvise freely, because healthcare has hard boundaries.
The hard problem is making the assistant natural and dependable at the same time.
I wrote about the architecture side of this in AI Voice Agent Architecture: What I Learned Building the Same Agent Three Times. The short version is that the realtime model should own the live conversation, while the surrounding system enforces the hard guarantees: identity checks, required fields, approved actions, escalation, and record fidelity.
I wrote about the testing side in LLM-as-a-Judge for Voice Agents. You cannot unit-test a conversation the way you unit-test a button. You need simulated callers, transcript review, judge calibration, replay testing, and regression checks that catch behavior drift.
That is also why AI software development breaks traditional software engineering. A small prompt change can affect every conversation path. Fixing one behavior can create a new failure three turns later in a totally different scenario.
Healthcare AI cannot rely on vibes.
It needs evals.
The maturity model for conversational AI in healthcare
One reason this category is confusing is that many products call themselves conversational AI while doing very different things.
Here is the maturity model I use.
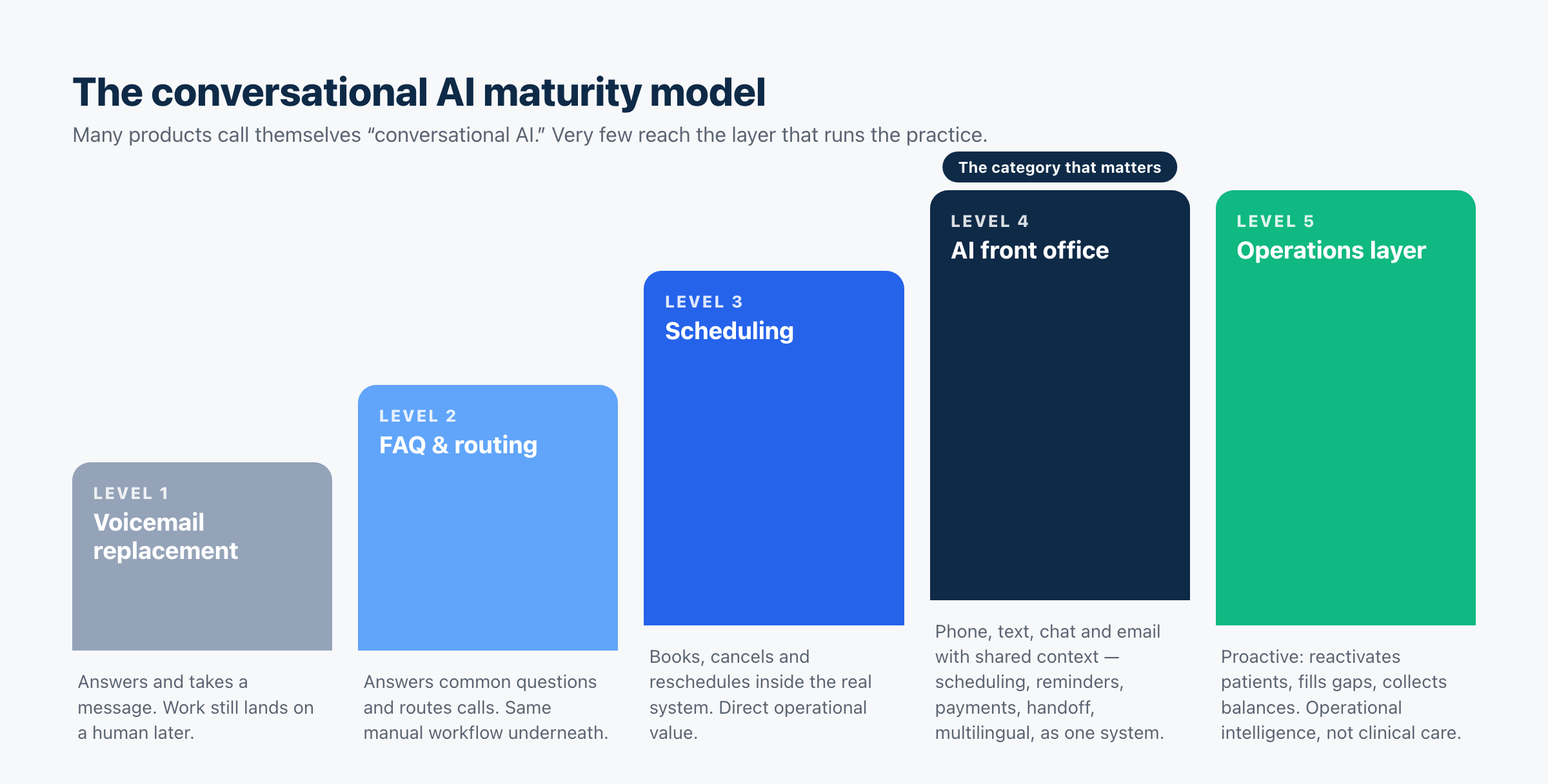
Level 1: Voicemail replacement
The AI answers, captures a message, maybe summarizes the call, and sends it to staff.
This is better than voicemail, but it is still passive. The work still lands on a human later.
Level 2: FAQ and routing assistant
The AI answers common questions, explains office policies, and routes calls.
This reduces interruption, but it still does not run the front office. It is mostly a conversational layer on top of the same manual workflow.
Level 3: Scheduling assistant
The AI can book, cancel, and reschedule appointments inside the actual system.
This is where the product starts creating direct operational value. The difference between “we will call you back” and “you are booked for Tuesday at 2:20” is enormous.
Level 4: AI front office
The AI operates across phone, text, web chat, and email with shared context. It handles scheduling, reminders, recalls, payments, intake, handoff, and multilingual communication as one system.
This is the category I care about.
It is not a phone bot. It is an operational layer.
Level 5: Healthcare operations layer
The AI becomes proactive.
It does not just respond when a patient reaches out. It identifies gaps in the schedule, reactivates lapsed patients, follows up on incomplete treatment, helps collect balances, detects workflow bottlenecks, and gives the practice leverage across the entire operational layer.
This is not autonomous clinical care.
It is operational intelligence.
What model builders still need to fix
Most of the work in building real AI front-office systems is compensating for gaps at the model layer.
If the frontier labs want to help the people building real healthcare agents, this is the list I would hand them.
Continue naturally after tool calls
When an assistant checks availability, looks up a patient, or triggers an action, the model often goes quiet unless the application pushes it forward.
In chat, that pause is hidden.
On a phone call, it becomes dead air. And dead air on a healthcare call feels like a dropped line.
A realtime model should know how to continue naturally after a tool call: “I’m checking that now,” “I found two openings,” “Let me confirm the details.” Builders should not have to hand-roll this behavior around every action.
Treat structured values faithfully
Times, dates, prices, balances, phone numbers, provider names, insurance IDs, and appointment types need to be rendered exactly.
A model should not round, paraphrase, or “clean up” structured values unless explicitly told to. “2:20” is not “around two.” “$148.75” is not “about $150.” A patient name is not a token to normalize.
Support required-field guarantees
In a real front office, some information is mandatory.
Before ending a call, the system may need name, date of birth, callback number, reason for visit, appointment type, insurance status, or consent for a payment link.
The model should support declarative required fields and validation rules. Not as prompt suggestions. As enforceable contracts.
Give confidence on names and numbers
Proper nouns and numbers are exactly where speech recognition struggles, and they are exactly where healthcare workflows are least forgiving.
Builders need confidence scores, alternative hypotheses, and better hooks for natural confirmation. The assistant should know when to say, “Let me make sure I got that right.”
Enforce instruction hierarchy
Healthcare agents need a safety floor the user cannot talk the model out of.
The patient should not be able to persuade the assistant to give clinical advice, skip identity verification, promise something outside policy, or perform an unauthorized action.
This cannot be solved by politeness. It has to be enforced.
Deliver real multilingual parity
A system that works beautifully in English and poorly in every other language is not a healthcare access product.
The assistant has to detect language, stay in language, switch when the patient switches, and preserve the same safety and accuracy guarantees across languages.
Translation bolted onto an English-first system is not enough.
How healthcare operators should evaluate an AI front office
The buyer’s question should not be, “Does it sound good?”
The buyer’s question should be, “Can I trust it with the operational front door of my practice?”
Here is the checklist I would use.
Can it take action inside the real system?
Can it actually book, cancel, reschedule, collect payment, and update the workflow? Or does it just create messages for staff?
A conversational AI that cannot act is an answering service.
Does it work across channels with shared context?
Phone, SMS, web chat, and email should not be four separate bots.
If a patient texts after calling, the assistant should know what happened. If the office follows up later, the conversation history should be usable.
Can it handle language access properly?
Can it serve patients in the languages they actually speak? Can it switch mid-conversation? Does it perform equally well outside English?
Language access is not convenience. For many patients, it is the difference between care and no care.
What are the clinical boundaries?
The vendor should be able to say clearly what the assistant will not do.
No diagnosis. No independent symptom triage. No medical advice. No unauthorized promises. No irreversible clinical action.
A vague answer here is a red flag.
What is the human handoff path?
Every AI front office needs a clean way to step back.
What happens when a patient is urgent, angry, confused, or clinical? Does the system transfer live? Create a priority alert? Escalate to the right role? Document why it escalated?
The handoff is not an edge case. It is part of the product.
How does it handle PHI?
Does the vendor sign a Business Associate Agreement? What PHI does it access? Where is it stored? How is access logged? What is retained? What is deleted? What downstream vendors touch the data?
A BAA alone does not make a product safe. But the absence of one is a warning sign.
How is reliability measured?
Ask what the vendor tests before deployment.
Do they simulate real callers? Do they test accents, noise, interruptions, language switching, appointment changes, angry patients, urgent calls, and incomplete information? Do they replay failures? Do they run regression tests after prompt changes?
If the answer is mostly “we monitor conversations,” that is not enough.
Monitoring catches failures after patients experience them. Evals catch failures before they ship.
What outcomes does it report?
A real AI front office should report operational outcomes, not just conversation volume.
Useful metrics include missed calls, booking conversion, appointments scheduled, reschedules handled, payments collected, recalls completed, average response time, escalation rate, staff time saved, patient satisfaction, and failure rates.
The point is not to sound human.
The point is to make the practice work better.
Why this is becoming urgent
AI adoption in healthcare is no longer theoretical. The AMA reported that 66% of physicians surveyed said they used healthcare AI in 2024, up from 38% in 2023. The same AMA survey found that 57% of physicians saw reducing administrative burden through automation as the biggest area of opportunity for AI.
Source: AMA — 2 in 3 physicians are using health AI
That is important because it shows where trust is forming first.
Physicians are not only asking for AI to diagnose. They are asking for AI to reduce the operational load around care: documentation, billing, notes, instructions, translation, summaries, patient communication, and other repetitive workflows.
But the same AMA report also shows the trust gap. Physicians cited needs like data privacy assurances, seamless workflow integration, training, feedback loops, and oversight.
That is exactly the bar the AI front office has to clear.
Healthcare does not need more impressive demos. It needs systems that fit into real workflows, protect patient data, maintain clinical boundaries, and improve access without creating new liability.
What this looks like in practice
This is the category we have been building at Viva AI.
Viva answers calls, texts, web chats, and emails for dental practices. It works 24/7, supports more than 100 languages, books directly into the practice management system, collects payments, sends reminders, runs recall and reactivation campaigns, and hands off urgent or upset patients to the human team.
It handles the operations around care.
It does not make clinical decisions.
In a published 30-day case study, one practice using Viva generated $30,877.30 in production, missed zero calls, maintained 90%+ patient satisfaction, handled 1,970 calls and 6,941 messages, and saved roughly 29–31 hours of staff time.
That is the kind of result that makes me believe the AI front office is one of healthcare’s first real conversational AI categories.
It is measurable.
It is operational.
It does not require AI to replace clinical judgment.
It improves access, reduces staff burden, and helps patients get to the right next step faster.
Dentistry is a particularly good proving ground because it has all the operational pain of healthcare with a faster feedback loop: high call volume, scheduling complexity, treatment follow-up, payments, insurance questions, recalls, and a clear link between front-office performance and production.
But the pattern is not dental-specific.
Primary care, urgent care, dermatology, physical therapy, optometry, behavioral health, and specialty clinics all have versions of the same problem. The clinical workflows differ, but the operational layer rhymes.
Patients need to get through. Staff need relief. Practices need the schedule to work. Communication needs to happen reliably, in the right language, on the right channel, at the right time.
That is the AI front office.
The bottom line
Conversational AI in healthcare will not win because it sounds human.
It will win when it becomes trustworthy infrastructure for patient access.
The front office is the right place for healthcare AI to become real because the work is high-volume, repetitive, measurable, and operationally important — but still bounded away from clinical decision-making.
That is the key.
AI should answer the phone, schedule the visit, send the reminder, collect the payment, translate the conversation, document the handoff, and escalate when needed.
Clinicians should make the clinical decisions.
When that boundary is clear, conversational AI stops being a gimmick and becomes infrastructure.
The future of healthcare AI is not only in the exam room.
A lot of it starts at the front desk.
Frequently asked questions
What is conversational AI in healthcare?
Conversational AI in healthcare is AI that communicates with patients through phone, text, web chat, or email. The best use cases today are operational: answering questions, scheduling, reminders, payments, intake, follow-up, and routing. Done correctly, clinical judgment stays with human providers.
What is an AI front office?
An AI front office is a conversational AI system that handles the operational entry points of a healthcare practice across channels, languages, and workflows. It does not just answer. It books, reschedules, collects information, sends reminders, collects payments, logs context, and hands off to staff when needed.
Can conversational AI replace a medical receptionist?
It can handle a lot of repetitive, high-volume work that overwhelms the front desk, especially calls, scheduling, reminders, and basic patient communication. But the goal should not be to remove humans from the practice. The goal is to remove busywork so humans can focus on patients, judgment, exceptions, and care.
Is conversational AI safe for healthcare?
It can be safe when built with clear boundaries: no diagnosis, no independent clinical triage, no medical advice, AI disclosure, human escalation, privacy controls, audit trails, and rigorous testing. A safe AI front office handles operations around care, not clinical decisions.
Why is the front office a good first use case for healthcare AI?
Because the front office is high-volume, repetitive, measurable, and operationally critical. Missed calls, long holds, poor language access, no-shows, and manual follow-up all affect patient access and practice performance. AI can help here without needing to replace clinical judgment.
What should practices look for in an AI front-office vendor?
Practices should look for integration with real systems, multi-channel support, multilingual performance, clear clinical boundaries, human handoff, HIPAA-aware data handling, Business Associate Agreements where required, audit trails, reliability testing, and outcome reporting beyond conversation volume.
Read next
- AI in Healthcare: A Builder’s Guide to What Actually Works
- AI in Healthcare: Real Examples That Work Today
- AI Voice Agent Architecture: What I Learned Building the Same Agent Three Times
- LLM-as-a-Judge for Voice Agents
- Why AI Software Development Breaks Traditional Software Engineering
- How AI in Dentistry Is Transforming Access and Prevention
Sources and further reading
- Healthy People 2030 — Access to Health Services
- Kyruus Health — Patient Access Journey Report
- KFF — Overview of Health Coverage and Care for Individuals with Limited English Proficiency
- HHS OCR — Language Access Provisions of the Section 1557 Final Rule
- Cochrane — Mobile Phone Messaging Reminders for Attendance at Healthcare Appointments
- AJMC — CAQH Index Finds $20 Billion in Cost Savings Opportunities
- AMA — 2 in 3 Physicians Are Using Health AI
- HHS — Business Associates
- NIST — AI Risks and Trustworthiness


